MYOFASICAL PAIN SYNDROMES - UNDERSTANDING MYOFASICAL
To fully understand fibromyalgia syndrome (FMS) and/or myofasical pain syndrome (MPS), one must have information and understanding of myofascia. Myofascia, a thin almost translucent film that wraps around muscle tissue, is the tissue that holds all the other parts together. It gives shape to and supports all of the body’s musculature. The myofascia can also be considered the “ground substance”. Myofasia can exist in a solid, semi-solid, or fluid state, and provides lubrication to surrounding muscle fibers, ligaments and tendons.
Inside the tiniest muscle fiber, myofascia wraps itself around each fiber. Bundles of fibers are then further wrapped with fascia, and eventually the entire muscle band and muscle group. The fascia continues to join, attach and blend itself into other structures including bone. These fascia layers may run lengthwise through the muscle, perpendicular and permeates through three-dimensionally around the muscle fiber.
The myofascia also helps to regulate circulation. The products of the body’s cellular functions and all the wastes from its cellular processing must pass through the connective tissue to reach the lymph and blood vessels. When the myofascia becomes affected biochemical messengers (hormones, and enzymes) don’t function properly. With accumulation of waste products, muscles receive insufficient fuel and oxygen leading to tightening of muscle tissue, local nerve ending irritation, and fascia thickening. This process can lead to pain, which results in further limited movement and more tightening propagating a vicious cycle.
Myofascial Pain Syndromes are considered local “soft-tissue” disorders that involve the myofasical tissue, the glue that holds together muscles, ligaments and other soft tissue structures. Myofascial pain syndromes are often caused by an initial injury, trauma or repetitive strain injury, and are maintained by one or more active trigger points and their associated reflexes.
- The Trigger Point is the actual tissue causing the Pain State (pain generator).
- Myofascial Trigger Points (MTrPs): May be active or latent.
An active Myofascial Trigger Point (MTrP) is a focus of hyperirritability in a muscle or its fascia that causes pain and tenderness at rest or with motion that stretches or loads the muscle. It prevents full lengthening of the muscle, as well as causing fatigue and decreased strength. Pressure on an active MTrP induces / reproduces some of the patient’s pain complaint and is recognized by the patient as being some or all of his or her pain.
A latent Myofascial Trigger Point does not cause pain during normal activities. It is locally tender, but causes pain only when palpated. It also refers pain on pressure. It can be associated with a weakened shortened more easily fatigued muscle.
MYOFASCIAL PAIN SYNDROMES – CLINICAL FEATURES
History of spontaneous pain associated with acute overload or chronic overuse of the muscle. The mildest symptoms are caused by latent MTrPs that cause no pain but cause some degree of functional disability. More severe involvement results in pain related to the position or movement of the muscle. The most severe level involves pain at rest.
- Spot Tenderness: A very tender small spot, which is found in a Taut Band.
- A taut band: A ropelike swelling found within the muscle probably due to sustained shortening of muscle fibers. Increasing the tension on the muscle fibers of the taut band can increase the sensitivity of the MTrP.
- Jump Sign: Pressure on the tender spot causes the patient to physically react to the precipitated pain by exclaiming or moving. This reaction indicates the level of tenderness but is also dependent on the pressure exerted by the examiner.
- Pain Recognition: Digital pressure on or needling of the tender spot induces / reproduces some of the patient’s pain complaint and is recognized by the patient as being some or all of his/her pain. This finding by definition identifies an active trigger point.
- Twitch Response: A transient contraction of the muscle fibers of the taut band containing the trigger point. The twitch response can be elicited by “snapping” palpation of the trigger point, or more commonly, by precise needling of the trigger point.
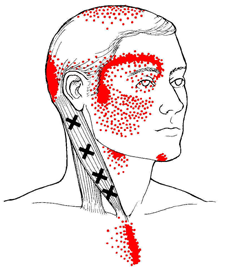
- Elicited referred pain: An active MTrP refers pain in a pattern characteristic of that muscle -Usually to a site distant to the MTrP. 85% of TrPs project distally. [The area of the referred pain is often tender and may contain satellite trigger points.] Latent TrPs also refer pain on pressure but usually require more pressure to do so.
- Restricted Range of Movement: Full stretching of the affected muscle is often involuntarily restricted by pain.
- Muscle Weakness: The patient is unable to demonstrate normal muscle strength on static testing of the affected side as compared to the opposite non-affected side. The involved muscle is also more easily fatigued.
PATHOGENIC FACTORS
Acute overload
- Overwork – Fatigue (Including postural stress)
- Chilling
- Gross Trauma
- Other Trigger Points
- Emotional distress
- Joint or nerve damage
- Visceral disturbance
Perpetuating Factors
- Mechanical: Structural Inadequacies e.g. the short leg syndrome, the small hemi pelvis, the long second metatarsal, short upper arms.
- Clothes. Tight constrictive clothing can produce MTrPs due to sustained muscle compression. E.g. Jeans related buttock pain, Bra strap headache, and wallet sciatica.
- Systemic. Metabolic, endocrine, toxic, inflammatory etc. Commonly found systemic factors include Hypothyroidism, folic acid and Iron deficiency.
- Toxic: alcohol.
- Metabolic – Inflammatory: gout.
- Relative Growth Hormone deficiency has recently been suggested as playing a pivotal role in MTrPs syndromes. (As growth hormone is necessary for muscle repair and its secretion is related to deep sleep which is frequently disturbed in patients with pain.)
Contact Us
13710 Olive Boulevard (Primary Office)
Chesterfield, MO 63017
Telephone: 314-469-PAIN (7246)
Fax: 314-469-7251
Exchange: 314-441-6965 (for after-hour Emergencies Only)
Hours:
Monday thru Friday
8:30 AM – 4:30 PM